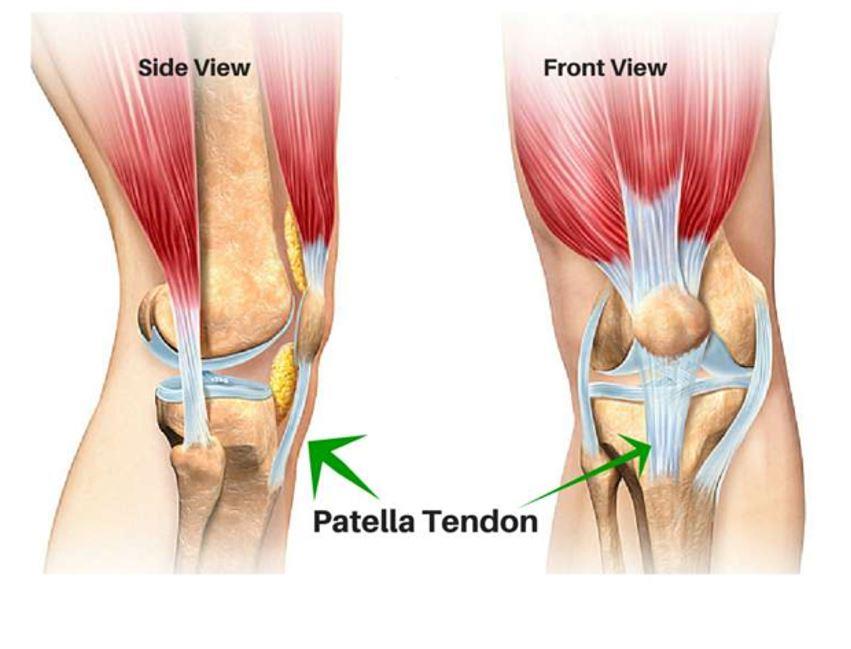
Patella Tendinopathy ( often called Jumpers Knee) is a common cause of knee pain both recreationally active people and athletes. This is particularly true for sports that involve repetitive side to side movements, quick stop starts and or rapid change of directions.
It is commonly seen in younger athletes, both in children and adolescents and increases in prevalence with age up to the ages of 18 years. It is more common in male athletes by 2x – 4x when compared to their
female counterparts.
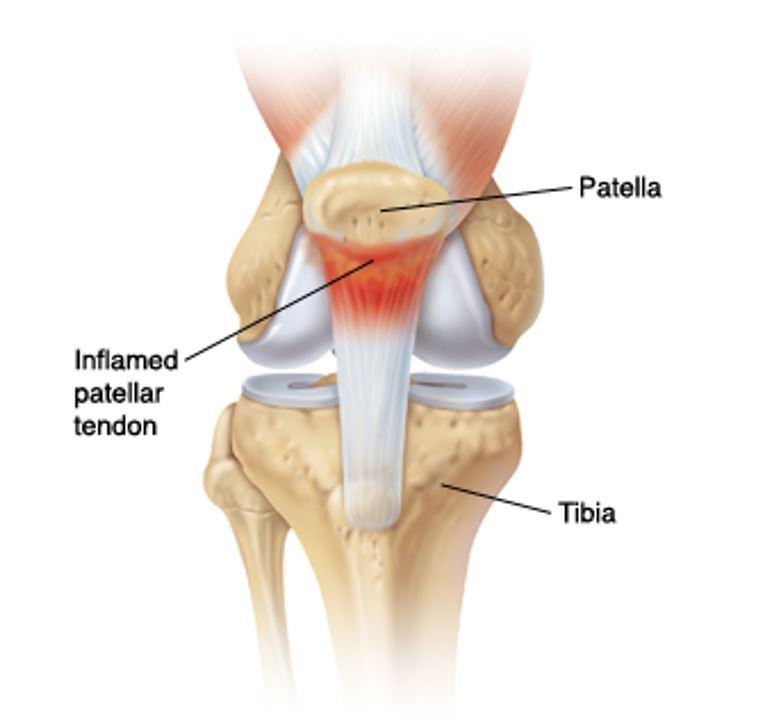
Characteristics of patella tendinopathy include pain and discomfort localised to the inferior pole of the patella (below the knee cap). It is often aggravated with movements such as jumping, landing, cutting and pivoting – these are known as high energy storage and release movements. Surfaces and choice of footwear can impact the amount of shock absorption as harder surfaces increase the risk of patella tendinopathy
There are a variety of different treatment modalities that can be applied to assist the rehabilitation of this injury. Treatment will depend on what stage of the tendon continuum the injury is sitting on, the severity of pain, the current loading patterns / amount of activity is involved and what planned on your sporting/ recreational calendar.
Majority of cases that are well managed and are in the settle well between 6-12 weeks pending the stage of tendinopathy along the continuum. These injuries may require continued management and vigilance depending on the athletic loads of the person but are often well self managed once the rehabilitation process has been engaged.
McKeon, J., Bush, H., Reed, A., Whittington, A., Uhl, T., & Mckeon, R., 2014 ‘Return-to-play probabilities following new versus recurrent ankle sprains in high school athletes’, Journal of Science and Medicine in Sport, vol. 17, No. 1. View link.
Our Clinic has been classified as an essential service to the community. We assist by trying to keep people healthy as possible and out of surgeries and decrease hospital admissions. At Inertia Health Group we are working hard to keep our patients and team members as safe as possible.
Due to our strict infection control procedures we have been deemed a low risk clinic- we have all completed the government COVID -19 Infection Control Risk Course and have implemented new waiting room procedures as well as intensified our cleaning procedures completing these regularly through the day. We have also implemented a virtual health service for those who require advice or assistance and cannot attend the clinic.
We appreciate our patients doing the right thing also!
Please call us with any questions or concerns 08 8359 2022.