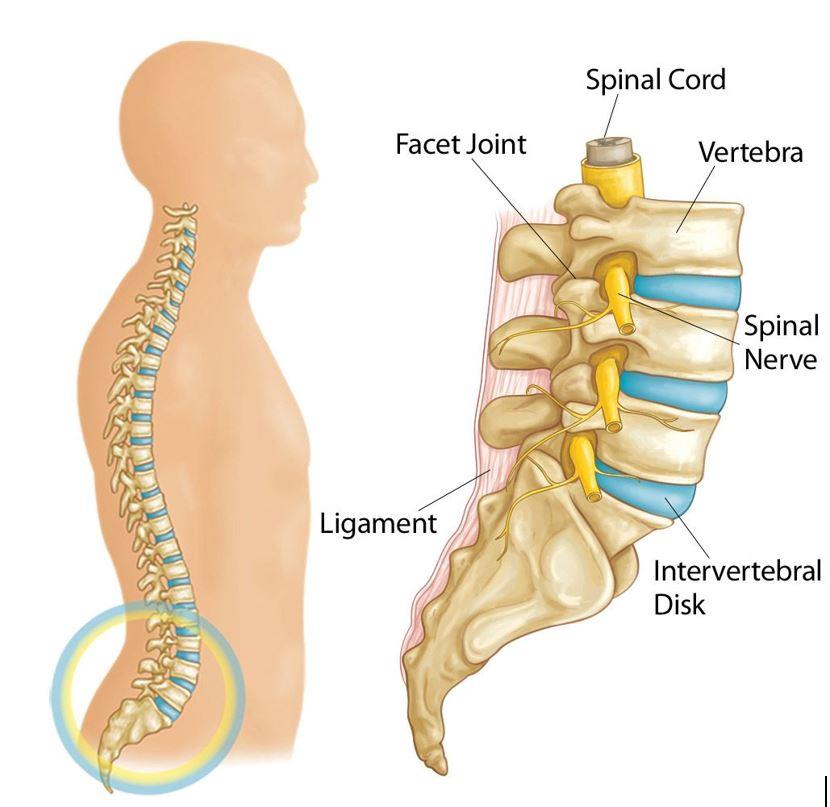
The lumbar spine refers to the 5 vertebrae in our lower back. Between these vertebrae lay intervertebral disc. These act as cushioning for the adjacent vertebrae and allow for movements of the spine such as flexion/extension, rotation and lateral flexion.
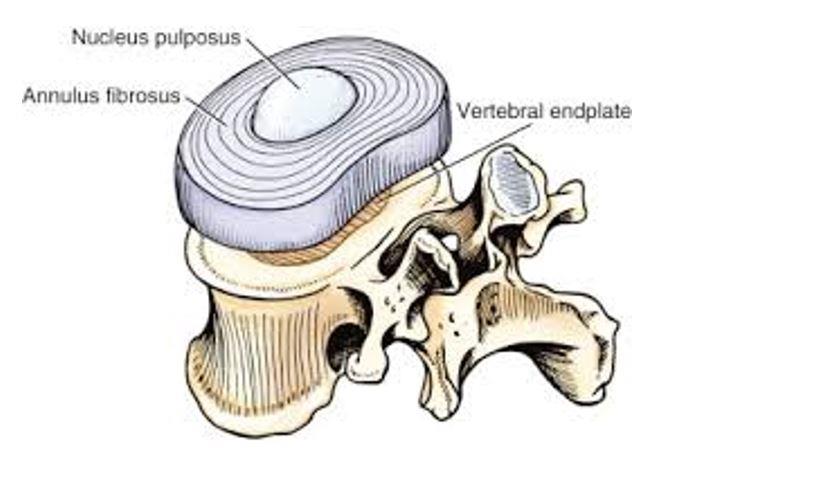
The disc itself is comprised of three main components as seen below:
Nucleus pulposus – This is a gel like substance at the center of the disc. When pressure is applied to it, it has the capacity to disperse in different directions.
Annulus fibrosus – Surrounding the nucleus pulpous is a strong band made from multiple layers of collagen fibers.
Vertebral endplate – A piece of cartilage that sits above and below the nucleus and annulus. It acts as a barrier between these structures and the bony vertebrae.
Lumbar disc herniation is a common cause of low back pain and can occur in varying degrees. A herniated disc is the displacement of disc material beyond the intervertebral space. In the Lumbar spine, this most commonly happens in a posterior direction (backwards) as most of our daily movements and postures involve flexing the lumbar spine.
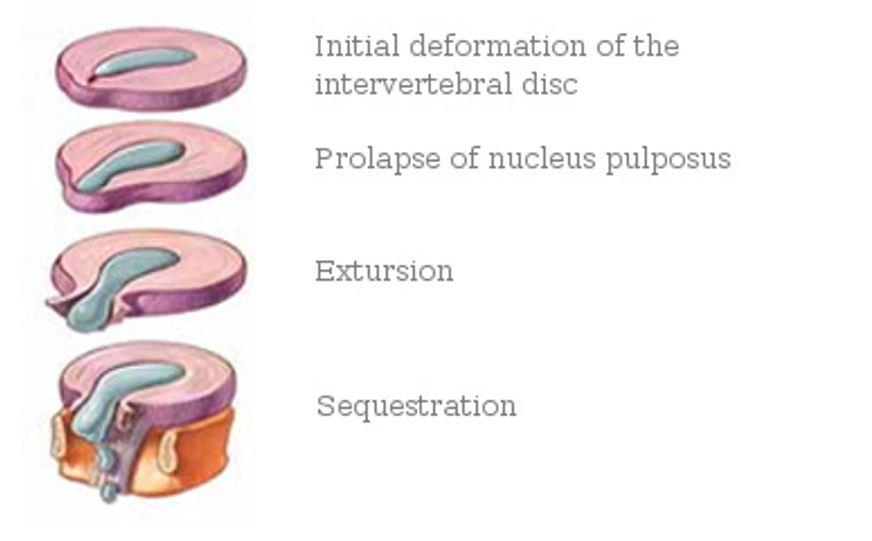
As described in the clinical anatomy of back pain (2006) there are four ways to classify disc herniations:
Just because you have been told you have a herniated disc; this may not be the cause of your pain. Disc herniation should be viewed as a normal part of aging, most people will have some level of disc herniation without back pain. A 2015 systematic literature review found that in 3110 individuals with NO BACK PAIN, disc herniation was present in a high number of individuals which increased with age:
Acute herniated discs commonly occur when bending forward to lift a heavy object. In these instances, pain can have a rapid onset and be far more severe and disabling. Even in these instances, significant rupturing of the annulus is rare. Muscles of the vertebrae will spasm as a protective mechanism which is a significant source of pain and limited movement in of itself. In these scenarios, discs have capacity to heal themselves, 75% of people will have a full recovery without any type of medical intervention within 6 months.
The initial phase of treatment is focused on protecting the injured site and managing the pain and spasm. This is best done by avoiding aggravating activities/postures, using medications such as pain relief or NSAIDS and relative rest (performing regular, gentle movements). Other modalities such as taping, ice or heat can also be of help. It is common for pain and spasm to worsen over the first 2-3 days after the initial injury as the body goes through its inflammatory process.
As a general guide, majority of people will see a good resolution to their symptoms within 4-6-week with Physiotherapy input. After this period, it is important to gradually re-introduce load to the affected tissues. While symptoms may largely be resolved, structures in the low back may exhibit increased neural sensitivity and muscles of the low back may have less conditioning due to the time spent in spasm. Re-occurring injury is common in this 6-12 week time frame as people increase their loads too fast, whether it be athletes continuing with their training regime or manual workers returning to full duties.
Your Physiotherapist will help your recovery by guiding your load management, providing manual therapy to reduce pain and stiffness and prescribing specific exercises to aid the healing process and progressive loading of the affected tissues. Your Physiotherapist will also help to prevent the re-occurrence of this injury by addressing potential underlying contributing biomechanical factors and providing advice regarding daily habits, posture, training and lifting techniques.
Brinjikji W, Luetmer PH, Comstock B, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811–816. doi:10.3174/ajnr.A4173
Jegede KA, etal. Contemporary management of symptomatic lumbar disc herniations. Orthop Clin North Am. 2010;41:217-24. PMID: 20399360 www.ncbi.nlm.nih.gov/pubmed/20399360.
Our Clinic has been classified as an essential service to the community. We assist by trying to keep people healthy as possible and out of surgeries and decrease hospital admissions. At Inertia Health Group we are working hard to keep our patients and team members as safe as possible.
Due to our strict infection control procedures we have been deemed a low risk clinic- we have all completed the government COVID -19 Infection Control Risk Course and have implemented new waiting room procedures as well as intensified our cleaning procedures completing these regularly through the day. We have also implemented a virtual health service for those who require advice or assistance and cannot attend the clinic.
We appreciate our patients doing the right thing also!
Please call us with any questions or concerns 08 8359 2022.