
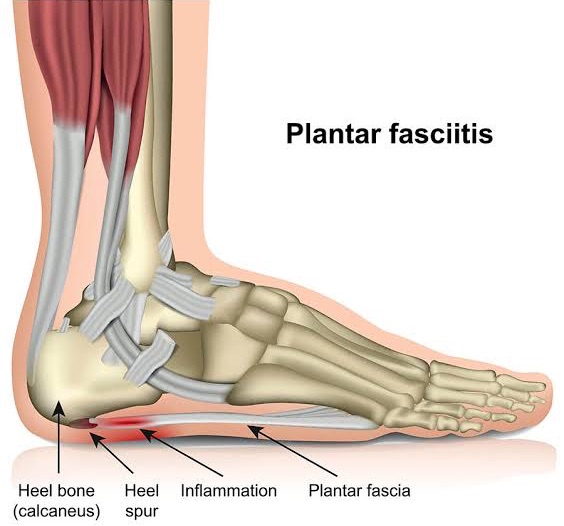
Plantar fasciitis, or heel pain as it is more commonly called, is the inflammation or degeneration of a structure within the foot called the plantar fascia (Schwartz, 2014).
The plantar fascia is a thick fibrous band that extends from your heel through to the base of your toes and functions to support the arch of your foot. It is thought that repetitive strain and overload from long periods of standing, activity, and a person’s foot type is the cause of this painful inflammation and/or degeneration (Schwartz, 2014).
Plantar fasciitis is one of the most common causes of foot pain and is estimated to effect 1 in 10 people during their lifetime (Riddle, Pulisic, Pidcoe, & Johnson, 2003). Plantar fasciitis can affect people in both sedentary and athletic populations, and anyone in between (Schwartz, 2014). However, research indicates that the peak incidence of the condition is amongst those aged between 45 and 64 years, and that it is more common amongst women. Those with either excessively flat, or high arched feet are also at an increased risk of developing plantar fasciitis (Riddle & Schappert, 2004).
Patients will usually present with a gradual onset of pain at the medial, or inner side of the heel (Lim, How & Tam 2016). This pain is often described as ‘first step pain’ and presents as severe pain occurring with the first few steps after rest, and then improving with movement. However, the pain may be re-aggravated by long periods of weight bearing (Schwartz, 2014). Clinically, palpation of the plantar medial heel will often result in tenderness, as will dorsiflexion of the first toe (Schwartz, 2014).
Unfortunately, not all cases of plantar fasciitis respond to conservative management. In sapproximately 5% of patients surgical intervention may be required (Lim, How & Tam 2016).
Cutts S, Obi N, Pasapula C & Chan W 2012, ‘Plantar Fasciitis’, Annals of the Royal College of Surgeons of England, vol. 94, no. 8, pp. 539-542.
Lim AT, How CH & Tam B 2016, ‘Management of plantar fasciitis in the outpatient setting’, Singapore Medical Journal, vol. 57, no. 4, pp. 168-171.
Riddle DL, Pulisic M, Pidcoe P & Johnson RE 2003, ‘Risk factors for plantar fasciitis: a matched case-control study’, Journal of Bone and Joint Surgery, vol. 85, pp. 872–7.
Riddle DL & Schappert SM 2004, ‘Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: a national study of medical doctors’, Foot Ankle Int., vol. 25, no. 5, pp. 303-310.
Schwartz EN, 2014, ‘Plantar Fasciitis: A Concise Review’, The Permanente Journal, vol. 18, no. 1, pp. 105-107.
Our Clinic has been classified as an essential service to the community. We assist by trying to keep people healthy as possible and out of surgeries and decrease hospital admissions. At Inertia Health Group we are working hard to keep our patients and team members as safe as possible.
Due to our strict infection control procedures we have been deemed a low risk clinic- we have all completed the government COVID -19 Infection Control Risk Course and have implemented new waiting room procedures as well as intensified our cleaning procedures completing these regularly through the day. We have also implemented a virtual health service for those who require advice or assistance and cannot attend the clinic.
We appreciate our patients doing the right thing also!
Please call us with any questions or concerns 08 8359 2022.