What are Stress Reactions & Stress Fractures?
Stress injuries are a large spectrum of injuries ranging from periostitis (inflammation of the periosteum – Sheath covering bones) to complete stress fractures with full cortical (bone) breaks. They are relatively common overuse injuries in athletes and are caused by repetitive sub-maximal loading on a bone over time. Most commonly, they occur in the lower extremities; stress fractures of the lower extremity account for 80-90% of all stress fractures. Upper extremity stress injuries are much less common. Stress fractures are common injuries among those individuals who participate in endurance and or high load- bearing activities such as running, cricket, military, and aerobic exercise.
How do Stress Reactions and Stress Fractures Occur?
Stress injuries reflect an imbalance between bone strength and its ability to tolerate the loads it endures. The imbalance can be due to fatigue, i.e., abnormal stress on normal bony architecture or insufficiency, meaning normal stress on the abnormal bone or the inability of the bone to recover well.
In healthy bone, osteoblastic (cells responsible for the laying down of new bone) activity repairs areas of trauma or injury, including that from physical activity. However, if the recovery period is not sufficient for osteoblasts to generate new bone, the rate of resorption by osteoclasts (cells responsible for degrading bone to allow remodeling) exceeds new bone formation, and thus, the bone weakens. Accumulated repetitively over time, this leads to stress reactions (inflammation within the bone), and if training is not modified, these become full-blown stress fractures.
Stress fractures occur due to overuse and/or overload when the rate of stress-induced microfractures exceeds the rate at which bone can repair.
Diagnosis of Stress Reactions and Stress Fractures
Stress fractures typically evolve with an insidious onset that typically occurs at the end of physical activity and has a focal point of tenderness. The pain usually progresses from pain with activity to persistent pain during activity and finally during daily activities and walking.
People usually describe a recent change or increase in physical activity or repetitive exercise with minimal recovery time. Physical examination typically identifies tenderness localised over the bony area, both with and without localised swelling.
Imaging of Stress Reactions and Stress Fractures
MRI imaging is the most effective at evaluating stress reactions and stress fractures, with an accuracy of approximately 88%. Bone scans are utilised in the diagnosis of stress fractures due to their ability to detect hot spots in bone. However, these are usually utilised if MRI is inconclusive or there are multiple suspected areas due to the significant exposure to radiation exposure to patients.
Grading Of Stress Fractures
Staging of stress injuries is based on MRI findings which are the most sensitive diagnostic modality. The MRI findings use the Fredericson classification system:
- Grade 1: Periosteal edema only
- Grade 2: Bone marrow edema (only on T2 weighted sequences)
- Grade 3: Bone marrow edema (on T1 and T2 weighted sequences)
- Grade 4: (4a) Multiple discrete areas of intracortical signal changes; (4b) Linear areas of intracortical signal change correlating with a frank stress fracture
You are also able to view periosteal reaction on x-ray, which typically correlates with a grade 3 stress injury on MRI, or a completed fracture line that correlates with a grade 4 stress injury. At this point, however, these stress fractures would be quite significant.
Your Physiotherapist or Podiatrist (for lower limb stress fractures) can also perform some special tests which may point to a specific diagnosis.
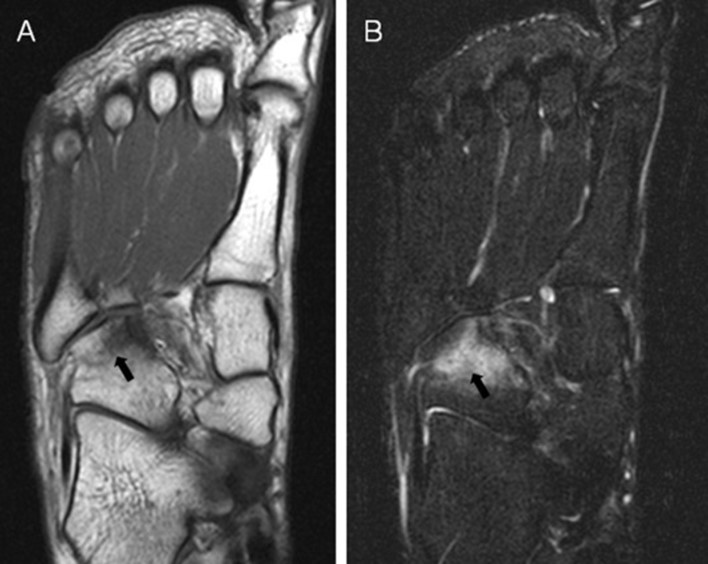
MRI image of increased signal (white areas) on the cuboid bone, which indicates a stress fracture. Contributed by Asia Pacific Journal of Sports Medicine.

Treatment & Rehabilitation of Stress Fractures
Physiotherapy and Podiatry Treatment of stress fractures requires identifying and modifying risk factors and load management initially.
Phase 1
Offloading Phase
You may benefit from complete offloading to allow the bone tissue to reduce the inflammation response in the bone. Your treating therapist can assist by devising an appropriate exercise plan for you during this time of offloading. They can also assist by providing manual therapy and dry needling to the area to ensure the tissue does not become tight and stiff during this time, as well as some gentle stretching to maintain the area’s range of movement with comfort levels.
Phase 2
Graduated Reloading Phase
This phase consists of gradual reloading of the tissue to ensure resilience is gradually rebuilt.
It is also a period of time when we can participate in a graduated strength and conditioning program to ensure the tissue and kinetic chain are functioning optimally as we build back into the sport. For lower limb stress fractures, your Podiatrist will be able to further investigate your foot biomechanics and may be able to prescribe a device to allow for optimal loading of the area as you return to activity and prevent further flare-ups.
Your Physiotherapist can also perform this role in dealing with stress fractures in the lower limb, back, and other areas in which they may present.
Phase 3
Graduated Return to Sport Phase
The graduated return to the sporting field. Again load management is critical in this phase of treatment as we want gradually expose it to normalised loads without eliciting another stress response.
When returning to the sport, this may look something like modified training sessions, limiting the distance of running at lower or higher intensities and slowly progressing at a pre-determined rate. Limiting the number of balls bowled per session or game. Restricting or controlling minutes played for a period of time before gradually increasing back to full minutes and full loads pending the response from the bone. Critical during this phase is also allowing enough recovery time between sessions to allow bony adaptations. This phase may look different for each individual based on the sport or workplace they are involved in and their individual responses.

Prognosis
These fractures have a variable healing time frame; some minor ones settle in 4-6 weeks, and some can be ongoing for 8 or 12 weeks, sometimes longer between 3-6 months.
Loading response needs to be monitored closely on resumption of loading to prevent re-aggravation of the injury. Patients usually have a very good outcome with conservative management of these injuries.
Common Stress Fracture sites include the following:
Metatarsals (long bones of the foot)
- Common in Dancers and ballet (2ND Metatarsal)
5th Metatarsal (outside of foot)
- Common in mid and long-distance runners (cross-country running)
- Common Military Personnel
Tarsals
- Navicular bone
- Common in sprinters, middle-distance runners, hurdlers, and basketballers.
Sesamoid Stress Fractures
- Common in runners, dancers, and gymnasts.
Tibia (Shin – shin splints or Medial Tibial Stress Syndrome)
- Common in Mid and long-distance runners and also in sports such as football and soccer.
- Common in Military Personnel
Fibula (outside leg bone)
- Common in Distance walkers, runners, jumping sports, and military
Pars Interarticularis Joints (Lower Back Vertebra)
- Common in Cricket players, particularly fast bowlers, also in gymnasts
Other Stress reactions or fractures:
Rib Stress Fractures
- Common in baseball, dancing, tennis, golf, rowing, backpacking, and windsurfing.
Patella Stress Fractures
- Common in Volleyball and Basketball, Jumping sports.
- Rare Stress Responses and Stress Fractures
Femoral Neck Stress fractures
Femoral Shaft Stress Fractures
If you are struggling with a stress response or a stress fracture and are uncertain about what you may be dealing with. Call our friendly admin team at the clinic on (08) 6244 2565 today or book online to get back on track!