
Iliotibial band pain is one of the primary sources of knee pain, particularly in runners’ lateral knee pain. Contrary to its name, ITB friction syndrome is a compression-based injury caused by thickening of the fascia of the lateral thigh. This fascia has many strong attachments to the femur and the patella. The ITB’s devotion to the lateral femoral condyle and the supracondylar ridge on the leg bone means the band is anchored firmly, suggesting no flipping or fractioning of the band over the hill. It is now recommended that the highly innervated tissue (with many nerve endings) between the ITB and the lateral femoral condyle experience compression forces as the knee moves through 30° of flexion and its peak tension is experienced. These compressions force illicit pain through the tissue in the area, causing aggravation, pain, inflammation, and an inability to continue.

How is iliotibial band pain present?
The type of pain that patients will usually present with iliotibial band pain or injury is localized tenderness over the femoral condyle (outside part of the knee). (See image above.) This pain is particularly noticeable as it moves through an arc of 25–35 degrees of flexion to extension (also known as the impingement zone). The pain on the lateral aspect of the knee can be reproduced as the hip extends while the knee flexes, which places an eccentric force (loading under lengthening) on the TFL. These loads are created in down-hill running environments or simply making your way down a flight of stairs.
What causes iliotibial band injuries?
Training load errors often cause iliotibial band injuries. What does this mean? It means these injuries are usually sustained by a population of people who rapidly increase their running or exercise volumes. It is even more particularly associated with an uptrend in downhill running books (trail runners or hill running tracks). Runners, exceptionally, can be more at risk of iliotibial band aggravation if running is performed with a narrow step width or if their running pattern has a higher volume of knee adduction (kneed falling into the midline), as this places more stress and strain on the ITB structure and also the anatomy of the lateral hip.
Interestingly, a person can mention biomechanics and a low relative tissue fatigue resistance capacity. Still, injury will not occur unless there is a rapid increase in applied training loads. However, one thing to note is that once this capacity level has been breached, the load capacity of the tissue itself is substantially reduced, and pain will ensue with relatively simple and non-challenging movements such as going down stairs or stepping off a gutter.
How long can ITB pain last?
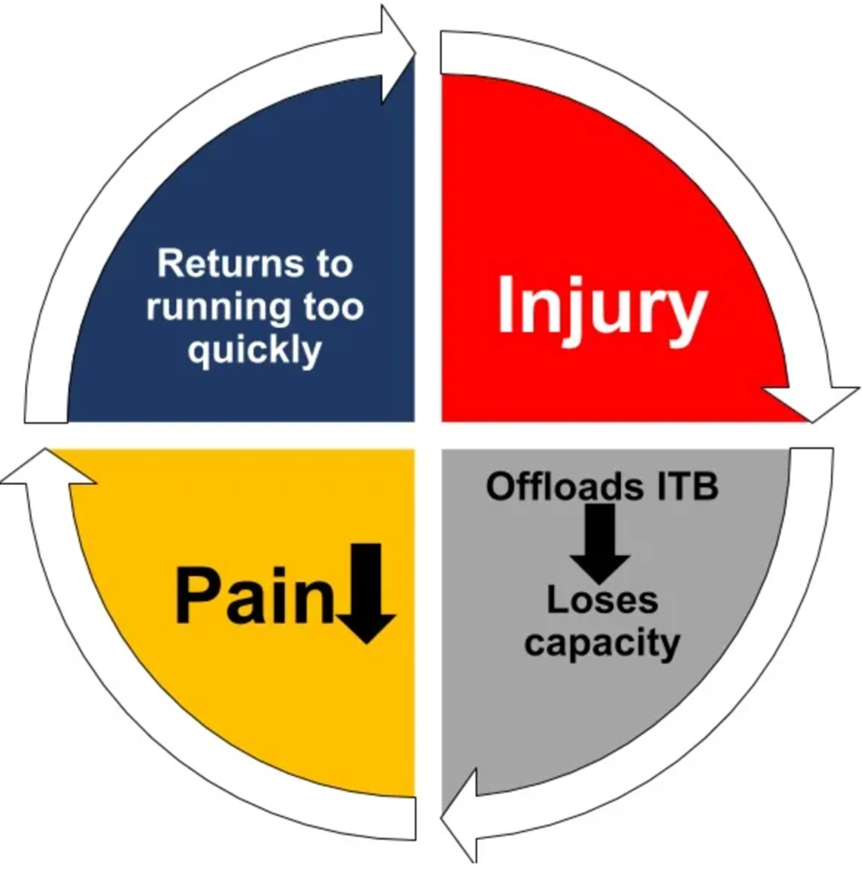
The tricky thing about ITB syndromes is that they can become persistent injuries, and there are several factors or reasons why:
- Runners or athletes often decrease or stop running completely when they first begin to suffer from ITB pain.
- This stress shielding causes the athlete or runner to lose more load capacity and tissue resilience (leading to weaker, more nonresilient tissue).
- As the pain begins to settle, the runner or athlete believes that the injury has improved and then returns to the activity they completed before the injury.
- The runner or athlete typically begins loading at the same rate they were pre-injury, and the training error repeats, resulting in more pain and loss of load capacity.
Is hip weakness a key contributor?
The short answer to this is yes. However, it is more found in individuals with ITB pain as opposed to being used as a predictor of who athletes will develop ITB pain. The research suggests that ITB pain causes hip weakness rather than vice versa. Researchers have hypothesized that compression of the highly innervated soft tissue between the ITB and the lateral femoral condyle (the adipose or fatty tissue we discussed earlier) inhibits the musculature around the hip. This affects or causes a maladaptive strategy to reduce compression forces acting on the tissue beneath the ITB. Despite these findings, we know that hip strengthening is critical in the success and resumption of regular activity and in rehabilitating these injuries.
Stay tuned, for in the next blog, we will discuss the treatment for these types of injuries in more detail!
Written By
Patrick Carbone
Doctor Of Physiotherapy
B.App.Sc. (Human Movement)
B.Ex.Sc. (Exercise Science)
References
- Baker RL, Souza RB, and Fredericson M. Iliotibial band syndrome: soft tissue and biomechanical factors in evaluation and treatment. PM&R. 2011;3:550-561.
- Fairclough J, Hayashi K, Toumi H, et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome Journal of Anatomy. 2006;208:309–316.
- Fairclough J, Hayashi K, Toumi H, et al. Is iliotibial band syndrome a friction syndrome? Journal of Science and Medicine in Sport. 2007;10:74–76.
- Hamill J., Miller R., Noehren B., and Davis I. A prospective study of iliotibial band strain in runners. Clinical Biomechanics. 2008;23:1018–1025.
- Hreljac A. Impact and Overuse Injuries in Runners. Medicine & Science in Sports & Exercise. 2004;845-849.
- Meardon SA, Campbell S, and Derrick TR. Step width alters iliotibial band strain during running. Sports Biomech. 2012;11:464–472.
- Messier SP, Edwards DG, Martin DF, et al., Aetiology of iliotibial band friction syndrome in distance runners Med Sci Sports Exerc. 1995;27:951–960.
- Noehren B, Davis I, Hamill J. ASB Clinical Biomechanics Award Winner 2006. Clinical Biomechanics. 2007;22:951–956.
- Orchard JW, Fricker PA, Abud AT, and Mason BR Biomechanics of iliotibial band friction syndrome in runners Am J Sports Med. 1996;24:375–379
- Rathleff MS, Rathleff CR, Crossley KM, and Barton CJ Is hip strength a risk factor for patellofemoral pain? A systematic review and meta-analysis Br J Sports Med. 2014;48:1088.
- Dr Richard Willy, Blog: Iliotibial Band Pain In the Runner, Aetiology & Assessment, Physionetwork, https://www.physio-network.com/blog/iliotibial-band-pain-in-the-runner-part-1-etiology-and-assessment/
- van der Worp MP, van der Horst N, de Wijer A, Backx FJ, Nijhuis-van der Sanden MW. Iliotibial band syndrome in runners: a systematic review Sports medicine. 2012;42:969–992.



