What is the general idea for rehabilitating people with ITB pain?

Generally speaking, the idea is to overload the injured tissue gradually. This sounds counterintuitive, but restoring and progressing the injured tissue’s tolerance is critical. It provides a stimulus to challenge the system and tissue to advance adaptation but not enough to further irritate the tissue by overloading its capacity.
Where does foam rolling fit in?
We often see foam rolling as a prescribed exercise as part of a mobility programme for people suffering from this condition. According to the literature, this effect is a brief change in flexibility. However, these only last a few minutes (concerning the ITB) and provide temporary pain relief, likely due to the quick change in central pain modulation (or the brain’s interpretation of pain or the tissue in the region). Rolling the lateral quadriceps (vastus lateralis), TFL (tensor fascia lata), and gluteals is more effective.
What about the treatment of ITB knee pain specific to runners?
When treating runners, it’s all about forces and running loads. The runner will typically experience a variation in running details. These can be broken down into three categories: a. high peak loads; b. including high levels of energy storage and release; c. cumulation of forces; this model of running staff has been adapted from Willy and Meira (2016). When rehabilitating the running athlete, all three loading components need to be addressed; this is how (see below).
- Peak loading is addressed through heavy, slow resistance training.
- Energy storage and release are addressed through plyometric-based exercise programming.
- Cumulative loading: incorporates a graded return to running programme
When designing running rehabilitation programmes, consideration needs to be given to the loading moments of the ITB through the running gait pattern of the individual.
Summary of Rehabilitation at each stage
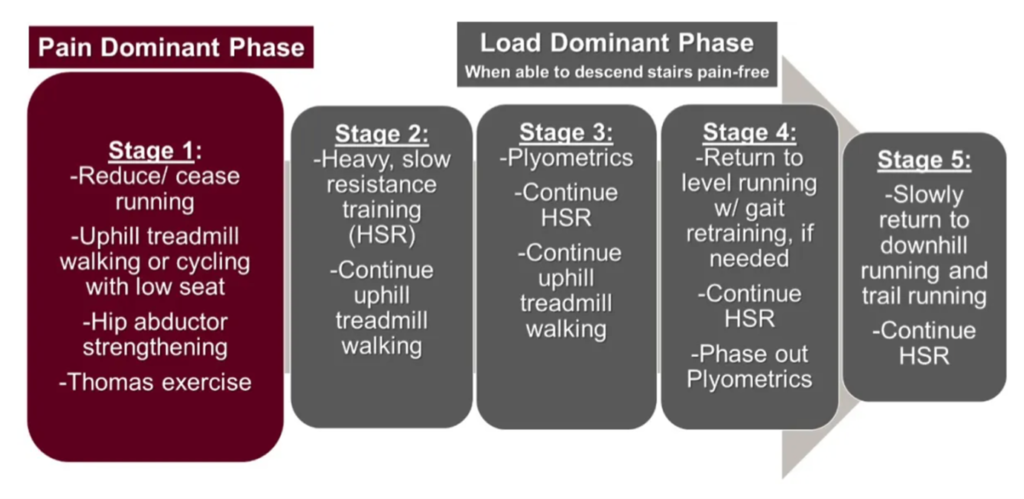
Stage 1: Pain-Dominant Phase
Goal: Reduce pain and irritation without reducing too much capacity
During this phase, load management is critical to reducing pain and irritation. Downhill loading and high-frequency stepping can be irritable; as such, the goal is to reduce the loading activities that are above the capacity of the tissue and cause irritation while maintaining as much loading as possible. Why? Loading is essential in pain processing, and it improves tissue quality.
We try to maintain activity levels as high as possible without exacerbating the affected tissue. This may mean reducing or ceasing running for the short term and replacing it with other non-irritating activities. Potential substitutes may be uphill walking, as it reduces energy storage and release of the ITB and can be performed outside of the impingement zone of the knee, and cycling with the seat further forward to ensure the knee is flexed to 35 degrees at the bottom of the pedal cycle to avoid the impingement zone. If these are not tolerable, swimming can be incorporated.
Example Rehab exercises in this stage may pertain to hip stability and mobility activities such as:
- Thomas’s hip flexor stretching
- Double- or single-leg bridging with or without banding
- Sidely leg lifting
- Side bridges from the knee and progressions
It is essential to understand why these may be prescribed or what aspects of the biomechanical chain are being worked on.
Loading Dominant Phases: Stages 2–5
Stage 2
Progression to these phases often depends on the patient being able to move down a flight of stairs with minimal to no pain. This part of rehabilitation programming is designed to concentrically and eccentrically load the relevant hip and quadriceps with heavy, slow resistance training via 4-6 second repetitions. An essential exercise in this phase is the split squat, which incorporates a progression of the stage one practises into a load-bearing and enhancing single approach. These loading exercises are essential for improving the load tolerance of the affected structures.
Stage 3
This phase will see the incorporation of plyometric loading exercises. This is now beginning to address the energy storage and release demands of the ITB and surrounding structures without the addition of repetitive running loading. This stage may last 1–2 weeks, pending the individual’s response, and is a bridge between locations. Examples of this stage are skater jumps due to the loading of the muscles responsible for hip stability, and these can progress to include resistance.
Stage 4
A return-to-running programme is beneficial to introduce at this stage. This must be graded and looked upon as a loading exercise rather than a fitness or conditioning exercise. It is a critical part of the rehabilitation process as, at this stage, the patient can become overzealous and re-injure or irritate through overload. A little pearl is regarding tweaking cadence by increasing it, as this can reduce overall time in the impingement zone.
Stage 5
This phase will see a gradual increase in training volume (running). Downhill running can be incorporated, as can trail running, should that be a goal. Strength training should continue once per week at this stage, pending the running loads.
- Boyer ER, Derrick TR: Select injury-related variables are affected by stride length and foot strike style during running. The American journal of sports medicine. 2015;43:2310–2317.
- Chaudhry H., Schleip R., Ji Z., Bukiet B., Maney M., and Findley T. Three-dimensional mathematical model for deformation of human fasciae in manual therapy The Journal of the American Osteopathic Association. 2008;108:379–390.
- Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy Br J Sports Med. 2009;43:409–416.
- Davis, I. Optimising the efficacy of gait retraining. BMJ Publishing Group Ltd. and the British Association of Sport and Exercise Medicine, 2018.
- Dye SF. The pathophysiology of patellofemoral pain: a tissue homoeostasis perspective. Clin Orthop Relat Res. 2005;100–110.
- Fairclough J, Hayashi K, Toumi H, et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome Journal of Anatomy. 2006;208:309–316.
- Fairclough J, Hayashi K, Toumi H, et al. Is iliotibial band syndrome a friction syndrome? Journal of Science and Medicine in Sport. 2007;10:74–76.
- Fredericson M, Wolf C. Iliotibial band syndrome in runners: innovations in treatment Sports medicine. 2005;35:451-459.
- Gabbett TJ. The training-injury prevention paradox: should athletes be training more brilliantly and complexly? Br J Sports Med. 2016;50:273-280.
- Gabbett TJ, Kennelly S, Sheehan J, et al. If overuse injury is a ‘training load error,’ should undertraining be viewed similarly? Br J Sports Med. 2016;
- Haggerty M., Dickin DC, Popp J., and Wang H. The influence of incline walking on joint mechanics Gait & posture. 2014;39:1017-1021.
- Hamill J., Miller R., Noehren B., and Davis I. A prospective study of iliotibial band strain in runners. Clinical Biomechanics. 2008;23:1018–1025.
- Khan KM, Scott A. Mechanotherapy: how physical therapists’ exercise prescriptions promote tissue repair British Journal of Sports Medicine. 2009;43:247-252.
- Koch JC. The laws of bone architecture American Journal of Anatomy, 1917, 21:177–298.
- Meardon SA, Campbell S, and Derrick TR. Step width alters iliotibial band strain during running. Sports Biomech. 2012;11:464–472.
- Noehren B, Scholz J, and Davis I. The effect of real-time Gait retraining on hip kinematics, pain, and function in subjects with patellofemoral pain syndrome. British Journal of Sports Medicine. 2010;45:691-696.
- Reiman MP, Bolgla LA, and Loudon JK A literature review of studies evaluating gluteus maximus and gluteus medius activation during rehabilitation exercises Physiother Theory Pract. 2012;28:257–268.
- Smith BE, Hendrick P, Bateman M, et al. Musculoskeletal pain and exercise—challenging existing paradigms and introducing new ones. Br J Sports Med. 2018;bjsports-2017-098983.
- Wiewelhove T, Döweling A, Schneider C, et al. A meta-analysis of the effects of foam rolling on performance and recovery Frontiers in Physiology. 2019;10:376.
- https://www.physio-network.com/blog/iliotibial-band-pain-in-the-runner-part-2-treatment/
- Willy R, Meardon S, Schmidt A, Blaylock N, Hadding S, and Willson J. Changes in tibiofemoral contact forces during running in response to in-field Gait retraining Journal of Sports Sciences. 2016;34:1602-1611.
- Willy RW, Buchanan L, Rogacki K, Ackerman J, Schmidt A, and Willson J. In-field Gait retraining and mobile monitoring to address running biomechanics associated with a tibial stress fracture Scandinavian Journal of Medicine and science in sports, 2016;26:197–205.
- Willy RW, Davis IS The effect of a hip-strengthening programme on mechanics during running and during a single-leg squat J Orthop Sports Phys Ther. 2011;41:625–632.
- Willy RW, Meira EP. Current Concepts in Biomechanical Interventions for Patellofemoral Pain. Int J Sports Phys Ther. 2016;11:877-890.
- Willy RW, Scholz JP, and Davis IS Mirror gait retraining for treating patellofemoral pain in female runners Clin Biomech 2012;27:1045–1051.



