Patrick Carbone
Doctor of Physiotherapy
Bachelor of Exercise Science
Bachelor of Human Movement and Health Science
What is a slipped disc?
Well, firstly, I need to correct you. This statement is not correct; discs do not slip. Whatever you have been told by your doctor, chiropractor, surgeon, physiotherapist, mum, dad, uncle, or great-aunt, you do not have a ‘slipped disc.’

What do the intervertebral discs in our backs do?
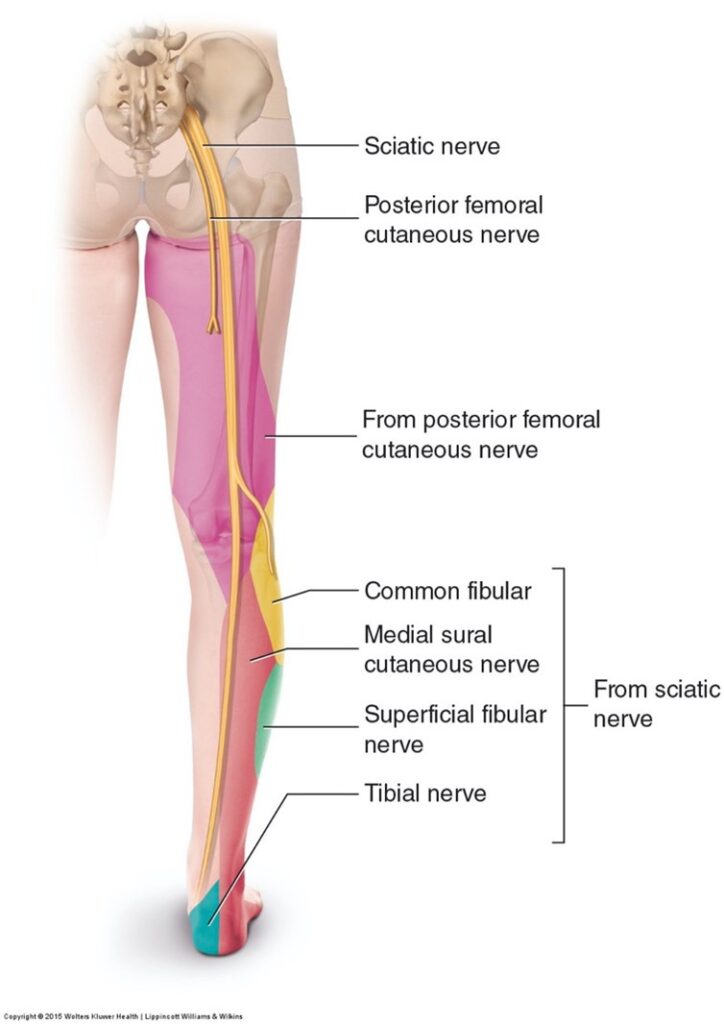
What discs do on scans is that they can herniate, prolapse, and bulge, but they most commonly become inflamed and irritated. Sometimes, when they prolapse or herniate (these terms are often used interchangeably), the nucleus of the disc or the jelly substance has the potential to compress a nerve as it exits the spine and pressure it in the foraminal canal (the hole in the vertebrae that allows the nerve to get to the spine). When this happens, you can experience pain and paraesthesia, or numbness, where pain can refer to the lower limb. This can also occur in the neck, referring to hand or arm pain. However, concerning the back, it is widespread. Lumbosacral radiculopathy is very common. On average, 3 to 5% of adults will experience symptoms in their lifetime. (Tarulli, AW, & Raynor, EM, 2007). L5 radiculopathy is the single most common lumbar radiculopathy because, in most instances, the L5 vertebrae are fixed on the pelvis and the L4 vertebrae move above it. This leads to significant shear forces over time, which can lead to discogenic change.
What may you experience when you have a slipped disc?
When someone has lumbar radiculopathy, 63% to 72% of them will feel paraesthesia, 35% will feel pain radiating down their leg, and 27% will feel numbness (Dydyk AM, Das, J 2020). Muscle weakness presents in up to 37%, absent ankle reflexes in up to 40%, and absent knee reflexes in 18% of patients (Dydyk AM, Das, J 2020). These are in symptomatic patients with nerve root compression; this injury is on the more severe end of the scale. However, it is interesting to note that about 27% of patients without back pain have been found to have disc herniation on MRI (Jensen, MC et al., 1994).
Disc disease is the underlying aetiology of less than 5% of patients with acute low back pain (Bogduk, N. 1991).
Are there different severities of a slipped disc or disc prolapse?
A slipped disc or disc prolapse causes three radicular symptoms and signs. Mild radiculopathy is considered a sensory loss and pain without motor deficits (inability to contract or use limb muscles), and moderate radiculopathy is a sensory loss or pain with a mild motor deficit. Severe radiculopathy is considered a sensory loss and pain with marked motor deficits (often, this form of injury may be sent straight for surgical opinion). The management of patients’ underlying symptoms will depend on the severity of the radiculopathy (Dydyk AM, Das, J 2020).
What is the physiotherapy treatment for a slipped disc or disc prolapse?
This is dependent on the severity of the injury. Often, patients who present with numbness, reduced spinal reflexes, and significant weakness will be referred to a spinal surgeon for an opinion. However, most of the time, people who suffer from disc bulges will significantly recover within 6–12 weeks with conservative management.
Conservative management is a combination of pain relief and anti-inflammatory medication initially to assist in inflammation reduction and ensure the patient can maintain mobility.
Treatment with your physiotherapist in Port Adelaide will consist of manual therapy (massage, joint mobilisation, myofascial release western acupuncture, dry needling, and cupping therapy) to assist in pain neuromodulation. Your physiotherapist will then devise a graduated mobility programme (stretching and gentle movement) with you and progress this along a continuum to where we can begin a graduated strength activation programme and build it into a loading programme. This may be seen by your physiotherapist or developed in conjunction with an Exercise Physiologist.
This is extremely important, as the research shows education regarding the condition and graduated exposure to loading exercises. Mobility is critical in reducing the capacity for developing chronic pain tracts and feedback loops, which ultimately leads to a long-term reduction in a person’s health. Early intervention for these types of injuries is critical for the person’s recovery in the long term.
What is the prognosis of a conservative or physiotherapy approach for a slipped disc?
Education is crucial for people who undergo this form of injury. Most cases of this will recover between 6 and 12 weeks, as most cases are mild to moderate. Care is to be taken within this time frame as well, as this time frame is known to have the highest rate of reaggravation if symptoms do not progress positively. This warrants further imaging studies and invasive treatments such as injection therapies or surgery. (Dydyk AM, Das, J 2020).
REFERENCES
Acute low back problems in adults: assessment and treatment Acute Low Back Problems Guideline Panel Agency for Health Care Policy and Research I am a famous physician. 1995 Feb 01;51(2):469–84.
Dydyk, AM, M Das J. Radicular Back Pain [Updated 2020, October 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020
Hall S, Bartleson JD, Onofrio BM, Baker HL, Okazaki H, and O’Duffy JD Lumbar spinal stenosis Clinical features, diagnostic procedures, and results of surgical treatment in 68 patients Ann Intern Med. 1985 Aug;103(2):271–5.
Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, and Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain Engl J Med. 1994 July 14;331(2):69-73.
Katz JN, Dalgas M, Stucki G, Katz NP, Bayley J, Fossel AH, Chang LC, Lipson SJ. Degenerative lumbar spinal stenosis: diagnostic value of the history and physical examination Arthritis Rheum. 1995 Sep;38(9):1236-41.
Tarulli AW, Raynor EM. Lumbosacral radiculopathy. Neurol Clin. 2007 May;25(2):387–405.



